Pyloric-sparing pancreatoduodenal resection: what is it? First days after surgery pancreatoduodenal resection (Whipple operation) When Whipple operation is necessary
Isolated lesions of the pancreas are rare. Combined injuries of the gland and other organs of the abdominal cavity are more often observed. Such injuries require urgent surgical intervention.
The abdominal cavity is usually opened with an upper midline incision and is approached to the pancreas through the gastrocolic ligament.
In the presence of bleeding from a wound of the pancreas, individual bleeding vessels are ligated with catgut. Often they resort to cutting off bleeding vessels through the gland tissue. After stopping the bleeding, the wound is cleaned, scraps of tissue are removed, crushed areas are excised and its edges are leveled. Then tamponade or suturing of the wound with catgut sutures is performed.
For superficial wounds of the gland, silk sutures are applied only to its capsule. The suture line is peritonized with a peritoneal sheet or an omentum, and gauze tampons are brought to the sutured wound.
If a part of the gland is crushed or incompletely detached, especially in the tail area, the wound is cleaned of blood clots, the crushed parts of the gland are excised and thorough hemostasis is performed. Then the wound surface of the resected section of the gland is stitched with continuous twisted or interrupted catgut sutures so that the sutures pass through the thickness of the gland to the entire depth of the wound. A second row of interrupted silk sutures is applied to the capsule and peritonization is performed with an omentum or peritoneal flap cut from the mesocolon transversum. Gauze tampons are brought to the sutured wound surface.
3 Operations for acute pancreatitis
Destructive forms of pancreatitis, complicated by abscess or necrosis of the pancreas, are subject to surgical treatment. To reduce the swelling of the gland, its capsule is dissected according to Korte. The abdominal cavity is opened with the upper midline incision, the gastrocolic ligament is dissected, and the anterior surface of the pancreas is exposed. The wound is expanded with mirrors and the abdominal cavity is carefully fenced off with gauze napkins. The capsule of the gland is dissected in the longitudinal direction and tampons are brought to the dissection site. SV Lobachev considers it expedient to make 4-5 sufficiently deep longitudinal incisions of the gland tissue from the head to the tail. If an abscess of the pancreas is found during the operation, then after opening it, pus is removed, as well as sequestered areas of the gland, and tamponade is performed.
4 Pancreatic resection: pancreatoduodenal resection
Pancreatoduodenal resection is the only radical treatment for cancer of the head of the pancreas, the preampular part of the common bile duct and the large nipple of the duodenum.
The operation consists in resection of the head of the pancreas and duodenum, followed by restoration of the patency of the gastrointestinal tract and biliary tract. Since the technique of pancreatoduodenal resection is very complex, many different variants of this operation have been proposed, differing in the methods of anastomosis between the bile ducts and the gastrointestinal tract, as well as in the technique of processing the pancreatic stump.
VN Shamov subdivides all methods of pancreatoduodenal resection into four groups.
The first group includes methods characterized by the imposition of an anastomosis between the gallbladder and the stomach and the stitching of the pancreas stump into the small intestine (Fig. 2).
The second group combines methods in which an anastomosis is made between the common bile duct and the small intestine; the stump of the gland is sewn into the small intestine (Fig. 3).
The third group is characterized by the imposition of cholecystojejunostomy with suturing of the pancreatic stump tightly or its extirpation (Fig. 4).
The fourth group is characterized by the imposition of an anastomosis between the common bile duct and the small intestine with the closure of the stump of the pancreas tightly or its removal (Fig. 5).
A rational arrangement of the anastomoses between the biliary tract, pancreatic stump, stomach and intestines is important for the outcome of the operation. Most often, the anastomosis is most high between the biliary tract and the intestine, somewhat lower - the anastomosis of the stump of the pancreas with the intestine, and even lower - gastroenteroanastomosis.
Operation technique. It is advisable to open the abdominal cavity with a transverse incision. If necessary, an additional midline incision can be made.
After opening the abdominal cavity, the duodenum and the head of the pancreas are mobilized. To do this, the parietal peritoneum is dissected outside the duodenum and the intestine is stupidly exfoliated together with the head of the pancreas from the retroperitoneal tissue and the inferior vena cava. Exposure of the anterior surface of the head of the pancreas begins with partial intersection of the omentum and gastro-colonic ligament, while ligating the right gastroepiploic artery. The mesentery of the transverse colon is pulled downward, and the stomach - upward, the parietal peritoneum is dissected and the mesenteric vessels are separated from the head and uncinate process of the pancreas. Then the pyloric part of the stomach is mobilized along the lesser curvature, the right gastric and gastro-duodenal arteries are ligated and crossed, displacing the duodenum and the head of the pancreas somewhat downward: the common bile duct and portal vein are isolated. At the level of the pylorus, the stomach is crossed between the imposed pulp and, spreading them apart, the neck of the pancreas is exposed.
Subsequently, a finger inserted along the upper edge of the pancreas bluntly separate the posterior surface of the neck of the gland from the portal vein. The gland at the level of the neck is crossed between the pulp. To avoid damage to the portal vein, a grooved probe or finger should be placed under the gland. The head of the gland is carefully pulled to the right, the adhesions are dissected, ligating and crossing the venous vessels going from the gland to the portal vein, as well as the lower pancreatic duodenal vessels. The hook-shaped process is removed from under the superior mesenteric vessels, crossing its ligament.
After that, the common bile duct is crossed. If for the removal of bile it is necessary to impose an anastomosis between the gallbladder and the small intestine, then the proximal end of the common bile duct is tied with two silk ligatures and the stump is carefully peritonized. For the final mobilization of the head of the pancreas, the ascending part of the duodenum is crossed, having previously bandaged the vessels going to it. The stump of the transected intestine is sutured and peritonized.
If it is necessary to completely remove the duodenum, the initial section of the jejunum is crossed. After that, the lower part of the duodenum is removed from under the superior mesenteric vessels, and the jejunal stump is subsequently used for anastomoses.
The mobilized head of the pancreas together with the duodenum is removed and a thorough hemostasis and peritonization of their bed are performed.
Then they start processing the stump of the pancreas. Most often, an anastomosis is applied between the stump of the pancreas and the jejunum. Such anastomosis can be made end-to-end or end-to-side. The first option is used less often, since the diameter of the stump does not always correspond to the intestinal lumen.
The technique of applying an end-to-side anastomosis is as follows. A loop of the jejunum is passed through the opening formed in the mesentery of the transverse colon. The stump of the gland is mobilized for 2 cm and a loop of the intestine is brought to it. Then the intestinal wall is dissected according to the transverse size of the gland and the first row of silk nodal sutures is applied to the posterior wall of the stump and the serous membrane of the intestine. With the second row of interrupted sutures, the posterior edge of the gland stump is sutured with the posterior lip of the lateral opening of the intestine. After that, in the same way, but in the reverse order, two rows of interrupted sutures are applied to the anterior wall of the anastomosis.
The technique of imposing an anastomosis between the stump of the pancreas and the small intestine in an end-to-end manner, as well as the technique of stitching the pancreatic duct into the small intestine using the Whipple method. Having finished processing the stump of the pancreas, they begin to impose an anastomosis between the common bile duct or gallbladder and the jejunum. Anastomosis is applied somewhat distal to the anastomosis of the pancreatic stump.
For the removal of bile, it is more advisable to produce choledochojejunostomy. This operation has a number of advantages over cholecystojejunostomy, since cholangitis and narrowing of the anastomosis are less common in the postoperative period. In addition, the risk of breakthrough of the stump of the common bile duct is excluded, which occurs with cholecystojejunostomy.
The imposition of such an anastomosis is not difficult with an enlarged common bile duct. However, if the bile duct is narrowed, then significant technical difficulties arise, in such cases it is easier to perform cholecystojejunostomy.
The next stage of the operation is to restore the patency of the gastrointestinal tract. To prevent the throwing of food masses into the bile and pancreatic ducts, the gastrointestinal anastomosis should be located below the imposed anastomoses with the bile duct and the stump of the pancreas.
The gastrointestinal junction can be applied end-to-end or end-to-side. In the first case, an additional interintestinal anastomosis is applied, in the second, the proximal end of the intestine is sutured tightly or sewn into the side of the bowel discharge loop. In some cases, when malignant neoplasms spread to the head, body and tail of the pancreas, it is extirpated. This operation is essentially a combination of two operations: pancreatoduodenal resection and resection of the body and tail of the pancreas.
The reconstructive stage of the operation during extirpation of the gland is facilitated by the fact that there is no need to impose an anastomosis between the gland stump and the small intestine.
Pancreatoduodenal resection is the only radical treatment for cancer of the head of the pancreas, the preampular part of the common bile duct and the large nipple of the duodenum.
The operation consists in resection of the head of the pancreas and duodenum with subsequent restoration of the patency of the gastrointestinal tract and biliary tract. Since the technique of pancreatoduodenal resection is very complex, many different variants of this operation have been proposed, differing in the methods of anastomosis between the bile ducts and the gastrointestinal tract, as well as in the technique of processing the pancreatic stump.
VN Shamov subdivides all methods of pancreatoduodenal resection into four groups.
The first group includes methods characterized by the imposition of an anastomosis between the gallbladder and the stomach and the stitching of the stump of the pancreas into the small intestine (Fig. 693).
693. Scheme of pancreatoduodenal resection. Option I.
The second group combines methods in which an anastomosis is made between the common bile duct and the small intestine; the stump of the gland is sewn into the small intestine (Fig. 694).

694. Scheme of pancreatoduodenal resection. Option II.
The third group is characterized by the imposition of cholecystojejunostomy with suturing the stump of the pancreas tightly or extirpating it (Fig. 695).

695. Scheme of pancreatoduodenal resection. Option III.
The fourth group is characterized by the imposition of an anastomosis between the common bile duct and the small intestine with the closure of the stump of the pancreas tightly or removing it (Fig. 696).

696. Scheme of pancreatoduodenal resection. Option IV.
A rational arrangement of the anastomoses between the biliary tract, pancreatic stump, stomach and intestines is important for the outcome of the operation. Most often, the anastomosis is most high between the biliary tract and the intestine, somewhat lower is the anastomosis of the stump of the pancreas with the intestine, and even lower is gastroenteroanastomosis.
Operation technique. It is advisable to open the abdominal cavity with a transverse incision. If necessary, an additional midline incision can be made.
After opening the abdominal cavity, the duodenum and the head of the pancreas are mobilized. For this, the parietal peritoneum is dissected outside the duodenum and the intestine is stupidly exfoliated together with the head of the pancreas from the retroperitoneal tissue and the inferior vena cava (Fig. 697, 698). Exposure of the anterior surface of the head of the pancreas begins with partial transection of the omentum and gastro-colic ligament, while ligating the right gastroepiploic artery. The mesentery of the transverse colon is pulled downward, and the stomach - upward, the parietal peritoneum is dissected and the mesenteric vessels are separated from the head and uncinate process of the pancreas (Fig. 699). Then mobilize the pyloric part of the stomach along the lesser curvature, ligate and cross the right gastric and gastro-duodenal arteries, displacing the duodenum and the head of the pancreas somewhat downward: the common bile duct and portal vein are isolated (Fig. 700).

697. Pancreatoduodenal resection. Mobilization of the right flexure of the colon.

698. Pancreatoduodenal resection. Mobilization of the duodenum according to Kocher. Blunt separation of the back wall of the intestine and the head of the pancreas from the underlying tissues.

699. Pancreatoduodenal resection. Detachment of the mesentery root of the transverse colon and parietal peritoneum from the head of the pancreas and the lower horizontal part of the duodenum.

700. Pancreatoduodenal resection. The small stuffing box is cut. Bandaging and crossing a. gastroduodenalis.
1 - lig. hepatoduodenale; 2 - a. gastroduodenalis; 3 - v. portae; 4 - ventriculus; 5 - lig. gastrocolicum; 6 - caput pancreatis; 7 - duodenum; 8 - duct us choledochus.
At the level of the pylorus, the stomach is crossed between the imposed pulp and, spreading them apart, the neck of the pancreas is exposed. In the future, a finger inserted along the upper edge of the pancreas, bluntly separate the posterior surface of the neck of the gland from the portal vein (Fig. 701). The gland at the level of the neck is crossed between the pulp (Fig. 702). To avoid damage to the portal vein, a grooved probe or finger should be placed under the gland. The head of the gland is gently pulled to the right, the adhesions are dissected, ligating and crossing the venous vessels running from the gland to the portal vein (Fig. 703), as well as the lower pancreatic duodenal vessels. The hook-shaped process is removed from under the superior mesenteric vessels, crossing its ligament (Fig. 704). After that, the common bile duct is crossed. If for the removal of bile it is necessary to impose an anastomosis between the gallbladder and the small intestine, then the proximal end of the common bile duct is tied with two silk ligatures and the stump is thoroughly peritonized (Fig. 705).
701. Pancreatoduodenal resection. The stomach is cut off and retracted to the left, the duodenal stump - to the right. Separation of the neck of the gland from the underlying portal and superior mesenteric veins.

702. Pancreatoduodenal resection. Intersection of the gland along a grooved probe.
1 - lig. hepatoduodenale; 2 - v. portae; 3 - a. hepatica communis; 4 - ventriculus; 5 - corpus pancreatis; 6 - mesocolon transversum; 7 - colon transversum; 8 - caput pancreatis; 9 - duodenum.

703. Pancreatoduodenal resection. Mobilization of the posterior surface of the pancreatic head. Ligation and transection of the venous vessels leading to the portal and superior mesenteric veins.
1 - lig. hepatoduodenale; 2 - v. portae; 3 - a. hepatica communis; 4 - ventriculus; 5 - v. lienalis; 6 - corpus pancreatis; 7 - v. mesenterica superior; 8 - mesocolon transversum; 9 - a. et v. pancreaticoduodenalis inferior anterior; 10 - colon transversum; 11 - caput pancreatis; 12 - duodenum.

704. Pancreatoduodenal resection. Dissection of the ligament of the hook-shaped process.
1 - lig. hepatoduodenale; 2 - a. hepatica communis; 3 - ventriculus; 4 - v. lienalis; 5 - corpus pancreatis; 6 - v. mesenterica superior; 7 - ligament of the hooked process; 8 - mesocolon transversum; 9 - colon transversum; 10 - a. et v. pancreaticoduodenalis inferior anterior; 11 - caput pancreatis; 12 - duodenum.

705. Pancreatoduodenal resection. Crossing the common bile duct.
1 - lig. hepatoduodenale; 2 - a. hepatica propria; 3 - v. portae; 4 - a. hepatica communis; 5 - v. lienalis; 6 - v. mesenterica superior; 7 - caput pancreatis; 8 - duodenum; 9 - ductus choledochus.
For the final mobilization of the head of the pancreas, the ascending part of the duodenum is crossed, after having tied up the vessels leading to it (Fig. 706). The stump of the transected intestine is sutured and peritonized.

706. Pancreatoduodenal resection. Intersection of the lower part of the duodenum.
1 - lig. hepatoduodenale; 2 - v. portae; 3 - a. hepatica communis; 4 - ventriculus; 5 - v. lienalis; 6 - corpus pancreatis; 7 - v. mesenterica superior; 8 - mesocolon transversum; 9 - colon transversum; 10 - caput pancreatis; 11 - duodenum.
If it is necessary to completely remove the duodenum, the initial section of the jejunum is crossed. After that, the lower part of the duodenum is removed from under the superior mesenteric vessels, and the jejunal stump is subsequently used for anastomoses.
The mobilized head of the pancreas together with the duodenum is removed and a thorough hemostasis and peritonization of their bed are performed.
Then they start processing the stump of the pancreas. Most often, an anastomosis is applied between the stump of the pancreas and the jejunum. Such anastomosis can be made end-to-end or end-to-side. The first option is used less often, since the diameter of the stump does not always correspond to the intestinal lumen.
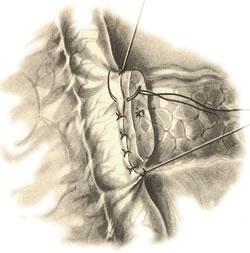
The technique of applying an end-to-side anastomosis is as follows. A loop of the jejunum is passed through the opening formed in the mesentery of the transverse colon. The stump of the gland is mobilized for 2 cm and a loop of the intestine is brought to it. Then dissect the intestinal wall according to the transverse size of the gland and impose the first row of silk interrupted sutures on the back wall of the stump and the serous membrane of the intestine (Fig. 707).

707. Pancreatoduodenal resection. End-to-side anastomosis between the gland stump and the small intestine. Suturing the intestine to the posterior wall of the gland stump.
The second row of interrupted sutures suture the posterior edge of the gland stump with the posterior lip of the lateral opening of the intestine (Fig. 708). After that, in the same way, but in reverse order, two rows of interrupted sutures are applied to the anterior wall of the anastomosis (Fig. 709, 710).

708. Pancreatoduodenal resection. End-to-side anastomosis between the gland stump and the small intestine. Suturing the posterior lip of the intestinal incision to the inner edge of the gland stump.

709. Pancreatoduodenal resection. End-to-side anastomosis between the gland stump and the small intestine. Suturing the anterior lip of the intestinal incision to the outer edge of the gland stump.

710. Pancreatoduodenal resection. End-to-side anastomosis between the gland stump and the small intestine. Suturing the anterior wall of the anastomosis with a number of interrupted serous-serous sutures.
Technique of end-to-end anastomosis between the pancreatic stump and the small intestine, as well as the technique of suturing the pancreatic duct into the small intestine according to the Whipple method are shown in Fig. 711, 712.

711. Pancreatoduodenal resection. A method of imposing an anastomosis between the stump of the gland and the small intestine in an end-to-end manner.

712. Pancreatoduodenal resection. The method of suturing the pancreatic duct into the wall of the small intestine according to Wyple.
Having finished processing the stump of the pancreas, they begin to impose an anastomosis between the common bile duct or gallbladder and the jejunum. Anastomosis is applied somewhat distal to the anastomosis of the pancreatic stump.
For the removal of bile, it is more advisable to produce choledochojejunostomy. This operation has a number of advantages over cholecystojejunostomy, since cholangitis and narrowing of the anastomosis are less common in the postoperative period. In addition, the risk of breakthrough of the stump of the common bile duct is excluded, which occurs with cholecystojejunostomy.
The imposition of such an anastomosis is not difficult with an enlarged common bile duct. However, if the bile duct is narrowed, then significant technical difficulties arise, in such cases it is easier to perform cholecystojejunostomy.
The technique of cholecystojejunostomy and choledochojejunostomy is given above.
The next stage of the operation is to restore the patency of the gastrointestinal tract. To prevent the throwing of food masses into the bile and pancreatic ducts, the gastrointestinal anastomosis should be located below the imposed anastomoses with the bile duct and the pancreatic stump.
The gastrointestinal junction can be applied end-to-end or end-to-side. In the first case, an additional interintestinal anastomosis is applied, in the second, the proximal end of the intestine is sutured tightly or sewn into the side of the bowel discharge loop.
In fig. 713 is a schematic representation of a complete Pancreatoduodenal resection.
713. Pancreatoduodenal resection in finished form (semi-schematic).
In some cases, when malignant neoplasms spread to the head, body and tail of the pancreas, it is extirpated. This operation is essentially a combination of two operations: pancreatoduodenal resection and resection of the body and tail of the pancreas.
The reconstructive stage of surgery during extirpation of the gland is facilitated by the fact that there is no need to impose an anastomosis between the gland stump and the small intestine.
On August 16, 2018, at the Vishnevsky Research Institute of Surgery, I underwent an operation with a very complex name pancreatoduodenal resection, which we will refer to as PDR.
This event was preceded by a story related to the discovery of a mass in the region of the head of the pancreas, which was found on ultrasound of the pancreas, confirmed by another ultrasound, MRI, MSCT, interpreted by radiologists from the Vishnevsky Research Institute, Blokhin Russian Cancer Research Center, and one more time endo ultrasound was identified. That is, with a very high probability of education there was.
In more detail about the period of detection, diagnosis and decision-making, I wrote and.
The operation is complex, without going into medical details, it is considered radical abdominal surgery. The team of the Department of Surgical Gastroenterology of the Vishnevsky Research Institute did it for 5.5 hours.
The essence of pancreatoduodenal resection
Well, that is, imagine, for 5.5 hours several people solved the problem of first disassembling a part of the digestive system, excising any excess, and then assembling it.
The first day after the operation, the person is in intensive care. I woke up around 14:00, 16.08. The head swam, there was no pain, oxygen was supplied to the nose, a tube protruded from the nose, which stretched into the stomach. For some reason.
From the right side two tubes hung down somewhere. Urine was also diverted by a catheter, which was, of course, where. A needle is inserted into the back, through which anesthesia is given, and here you are, with all this, you come to your senses.
There was no escape from anesthesia as such, I did not feel sick, although, as I read it happens.
The sisters come up regularly, the thing on the arm constantly measures the pressure, the night passed in oblivion, but even seemed to be asleep.
From the intensive care unit they transfer to the next day, if no complications happened, in my case, apparently, it did not happen, and at about 12 on about 17.08 a gurney arrived with two sisters from the department, who taught me to crawl from the intensive care gurney to the department gurney. The procedure is called Booty Shoulders.
The first day after resuscitation.First, they brought me to the dressing room, changed the dressings, then placed me on the bed in the ward, the first painful sensations appeared in the wound area - the constant supply of anesthesia was stopped and remained in intensive care.
On the first day, I used the service of an individual nursing post - this is when a nurse personally looks after you, who gives you the basic basics of what to do in a given situation after the operation. Well, it helps to get dressed in elementary, turn your neck.
About 2 hours after being placed in the ward, it began to sausage from pain, it felt like the cat Health was sitting in its stomach and twirling and scratching. It ended up with a pump with painkillers brought in and life started to improve again.
Until the evening, you just lie there and drip anesthetic on one side, and on the other - some other dropper.
Then two doctors came and said: lying is bad. Walking is good. Together they put me in a sitting position and told me to "get up and go."
But what, I say, I read on the Internet that after this operation people are in intensive care for several days, and then a few more in the ward.
Well, I began to walk. On the first evening after being placed in the ward. Because the movement forms the blood flow and prevents any stagnation there.
The hardest part is getting up and going to bed. You are in a bandage all the time, "tails" dangle on the right - these are drainage tubes through which they look at what goes into the peritoneum and whether there is blood flow. No food.
We began to drink and the task was to let urine in a natural way by the evening of the first day, because the drainage should be natural. It turned out, but the first moments are hard, because there was a catheter.
Terrible to sleep. Because on the back. Because any movement is painful, though not much. Constant pain relief does the trick.
The second and next days after resuscitation.On the second day, you have to walk even more. Drink even more. We must start eating. I already manage to get up and go to bed myself. Drinking yogurt was used, in the evening of the third day after the operation, I began to eat porridge.
The temperature is 37.3-37.7, sugar jumped to 16, calmed down with a dose of insulin. This is how a disturbed gland behaves, from which a piece was chopped off. And she will behave strangely for a while.
In the hospital every weekday morning a round trip. The head of the department and the attending physicians ask questions, look at the drains, temperature and some kind of observation. According to the schedule, nurses pierce pharmaceutical support - I have three types of supportive drugs, on the third day they turned on an antibiotic, additional anesthesia at night. And all the time, politely and attentively. It just really impresses me in this hospital.
On the 4th day I had an Uzi. Like the rules. Doctors say norms. The condition is improving. They removed one drain.
On the 6th day, the second drainage was removed, during the day the temperature is slightly 37.3-37.5; it falls by the evening, in the morning it is not. They say it will pass.
The complication control stage is in progress. This operation has a rather high probability of all sorts of complications, which, of course, I would like to avoid, but for now we are watching.
At the same time, doctors begin to troll about whether it’s time for me to go home, it’s too brisk to move.
The cut out something went to histology, we are waiting for another week. The operation went on as planned, nothing supernatural was visually found.
In Vladimir, friends and Olga are looking for a gastroenterologist, whom I want to hire as a personal doctor who will understand my body, the situation and will accompany from the point of view of rehabilitation everything that surgeons had to intervene in.
Depending on the results of histology, if necessary, we will draw up an action plan in the direction of oncology.
Well, a little later I will start planning my motor rehabilitation.
When I made the decision to do this operation, I could hardly find anywhere descriptions of how the first days of recovery go and, as my own experience now shows, nothing really terrible happens. And it is scary when there is no understanding.
We continue to continue. Here.
UPD: I spent 23 working days in the hospital. In itself, the recovery after the operation took about 9 days, as a result of which the wound had already healed, the stitches were removed and it was possible to be discharged, but then the body turned on the temperature for a week, and 7 days later gastrostasis happened - this is a suspension of gastric motility.
This is one of the most common complications following PDD surgery and is not critical if under medical supervision. It took 3 days.
9658 0
Mobilization of the duodenum. After crossing the intrinsic ligament of the uncinate process, the entire complex proposed for resection is held at the junction with the stomach and on the lower horizontal portion of the duodenum. Be very careful not to damage a. colica media of the Riolan arcade of the colon, the distal part of the duodenum and the initial part of the small intestine are most prominent.
The duodenum is maximally secreted together with the pyloric section of the stomach. Recently, there has been a tendency towards pyloric surgery. The lesser omentum is crossed between the clamps in such a way as to remove the lymph glands as much as possible. This sometimes requires preliminary ligation of the left gastric artery, departing from the stomach wall by 2-3 cm. A clamp is applied to the duodenum near the pyloric section or directly on it.
A clamp is also applied proximal to it. It is best to apply stapling devices, which facilitates the isolation of the resected section of the duodenum together with the head of the pancreas. For better observance of asepsis, rubber caps are put on the crossed duodenum (A.A. Shalimov). This makes it easier to pass it in the area of \u200b\u200bthe trait ligament into the lower abdominal cavity through the mesocolon of the transverse colon.
Some surgeons perform this part of the operation in reverse order. First, the loop of the small intestine is crossed distal to the Treitz ligament, and then the proximal end is transferred above the mesocolon. The entire resected duodenopancreatic complex is removed. A thorough final hemostasis is performed, washing a large wound surface with antibiotic solutions dissolved in 0.25% novocaine solution or saline solution (500.0 ml). Taking into account the large volume of the operation, it is obligatory to return blood from the wound with the Fresenius apparatus. The general view of the operating wound after the end of the first organ-carrying stage of pancreatoduodenal resection is shown in Fig. 105.
Fig. 105. Pancreatoduodenal resection. General view of the operating field after the end of the first stage of the operation:
1 - common bile duct; 2 - portal vein; 3 - inferior vena cava; 4 - aorta; 5 - own hepatic artery; 6 - splenic artery; 7 - stump of the tail of the pancreas; 8 - spleen; 9 - superior mesenteric artery; 10 - pancreatoduodenal artery; 11 - lower pancreatic artery; 12 - transverse colon; 13 - bringing down the stomach; 14 - end of the small intestine; 15 - gallbladder
From this moment, the restorative and reconstructive, or second main, stage of the operation begins. There are about 200 methods for its implementation. However, their essence boils down to five basic principles.
The first stage of reconstruction is restoration of pancreatic juice outflow along the Wirsung duct, or its complete blockage. Their options are different (Fig. 106).

Fig. 106. Options for processing the stump of the tail of the pancreas during pancreatoduodenal resection:
a - anastomosis with the discharge loop of the small intestine distal to the gastroenteroanastomosis; c - suturing tightly or pyombating the duct; c - the formation of gastropancreatic anastomosis; d - terminal pancreatojejunostomy; 1 - common bile duct; 2 - stomach; 3 - sutured loop of the small intestine; 4, 8 - sutured tail end of the pancreas; 5 - gastroenteroanastomosis; 6 - pancreatojejunostomy; 7- pancreatogastroanastomosis
Then a system of anastomoses is performed: pancreatojejunoanastomosis, choledochojejunoanastomosis, jejunogastroenteroanastomosis, jejunojejunoanastomosis, cholecystojejunoanastomosis, and separate methods of pancreatoduodenal resection are distinguished. They are formed in the following order: pancreatojejunoanastomosis, jejunogastroanastomosis, choledochojejunoanastomosis with cholecystectomy, Brown's fistula between bowel loops for unloading (Coli, 1943) and are presented in Fig. 107.

Fig. 107. Pancreatoduodenal resection. Operation Coli (1943): 1 - gallbladder; 2 - common bile duct; 3 - stomach stump; 4 - gastrojejunostomy; 5 - the stump of the pancreas; 6 - pancreatojejunostomy; 7 - disabled loop of the small intestine according to Roux; 8 - jejunojunoanastomosis; 9 - loop of the small intestine; 10 - choledochojejunostomy
The second stage - a disconnected loop of the small intestine according to Roux is formed, and then two of the above anastomoses are created with it (there are 7 variants of operations according to Whipple, 1947), one of them is shown in Fig. 108.

Fig. 108. Pancreatoduodenal resection. Operation Whipple (1947):
1 - a loop of the small intestine, brought to the stump of the tail of the pancreas; 2 - the tail of the pancreas; 3 - common bile duct; 4 - stump of 1/2 of the resected stomach; 5 - gastrojejunostomy with a disconnected loop of the small intestine according to Roux; 6 - jejunojunoanastomosis; 7 - disabled loop of the small intestine according to Roux; 8 - pancreatojejunostomy; 9 - choledochojejunostomy
The third stage - instead of choledochojejunostomy, an anastomosis with the gallbladder is used (Fig. 109).

Fig. 109. Variant of the restorative-reconstructive stage of pancreatoduodenal resection (according to Sessaga, 1948):
1 - hepatic duct; 2 - common bile duct; 3 - stomach; 4 - gastroenteroanastomosis; 5 - pancreatoentero anastomosis with the tail of the pancreas; 6 - Brownian anastomosis; 7 - the discharge end of the small intestine; 8 - loop of the small intestine; 9 - cholecystoenteroanastomosis
The fourth stage - the tail of the pancreas and its ducts are blocked and anastomoses with hollow organs are not formed, or the rest of the anastomoses can be performed in various, rather complicated versions (Fig. 110, 111).

Fig. 110. A variant of blocking the tail of the pancreas without anastomosing it with hollow organs: 1 - common bile duct; 2 - stomach; 3 - the tail of the pancreas; 4 - discharge disconnected loop of the small intestine along Roux; 5 - jejunojunoanastomosis; 6 - leading loop of the small intestine; 7 - sutured end of the tail of the pancreas (according to Kochiashvili, 1964)

Fig. 111. Reconstructive stage of pancreatoduodenal resection according to V.V. Vinogradov (1964): 1 - common bile duct; 2 - stomach; 3 - the tail of the pancreas; 4 - pancreatojejunostomy; 5 - gastrojejunostomy; 6 - outlet end of the loop of the small intestine; 7 - choledochojejunostomy; 8 - gallbladder
The fifth stage - simplified methods of reconstructive operations with anastomosis of the tail of the pancreas with the stomach through the posterior wall according to M.P. Postalov et al. (1976) or with a single loop of the small intestine (Fig. 112).

Fig. 112. Reconstructive stage of pancreatoduodenal resection with preservation of the pyloroduodenal zone:
a - the formation of pancreatic anastomosis distal to the gastroenteroanastomosis; b - pancreatojejunoanastomosis proximal to gastroenteroanastomosis; c - pancreatojejunostomy with a disconnected loop of the small intestine according to Roux
In the first variant it is necessary to perform a whole system of anastomoses (MI Kuzin, MV Danilov, DF Blagovidov, 1985). Therefore, operations are lengthy and traumatic.
In the second variant, anastomosis is performed with the Roux-en-route loops of the small intestine disconnected. There may be a separate anastomosis with the stump of the stomach or choledochus, pancreas. We believe that this technique is the most progressive, but it is currently used quite rarely.
In the third variant, anastomosis is performed with the gallbladder and the loop of the small intestine. However, there is always uncertainty about the adequate outflow of bile through the cystic duct. In addition, the presence of an inflammatory process in the bladder sometimes contributes to the formation of calculi in it, which block the cystic duct. This technique is used as a way out.
In the fourth variant, it is always necessary to bring drains to the sutured stump of the pancreas for constant aspiration.
In the fifth variant, one disconnected loop of the small intestine along Roux is formed and all the necessary anastomoses are formed with it (modification of the Whipple operation) (Fig. 113). A feature of this operation is that 1/2 of the stomach is resected. This loop is passed behind the transverse colon. Recently, a disabled Roux loop has not been used, but simply anastomoses are formed with a bowel loop held behind the transverse colon. This greatly simplified the operation. The technique of this operation is as follows.

Fig. 113. Modification of Whipple operation (a, 6 - reconstructive stage of the operation):
1 - stomach; 2 - common bile duct after cholecystectomy; 3 - stump of the resected 1 / 3-1 / 2 stomach; 4 - pancreatojejunostomy (with the tail of the gland); 5 - gastroenteroanastomosis; 6 - transverse colon; 7 - loop (outlet end) of the small intestine, below the mesocolon; 8 - the end of the discharge loop of the small intestine; 9 - choledochojejunostomy
After removal of the complex of the head of the pancreas and duodenum through the mesocolon, the small intestine is harvested and, if possible, mobilized as much as possible and carried through the mesocolon to the stump of the pancreas. According to this principle, anastomoses have recently been used with preservation of the pyloric pulp (Fig. 114). The options for these operations are different. The main doubt in the use of such anastomoses is the high possibility of developing peptic ulcers.

Fig. 114. Pancreatoduodenal resection. Pilorosaving operation: a - the estimated volume of resection; b - resected complex of the pancreas and duodenum; 1 - duodenum; 2 - common bile duct; 3 - the stump of the cystic duct; 4 - pyloric stomach; 5 - pancreas; 6 - stump of the tail of the pancreas (red dotted line shows the volume of the operation)
When forming a choledochojejunoanastomosis, we always remove the gallbladder beforehand, and the choledoch, departing from the stump by 1 cm, dissect longitudinally to increase the perimeter of the anastomosis (Fig. 115).

Fig. 115. Scheme of the formation of choledochojejunal anastomosis:
a - undesirable; 6 - with an increase in the perimeter of the anastomosis
When forming a pancreatojejunal anastomosis, we use the invagination principle. The pancreas is separated from the tissues by no more than 1.0 cm, so as not to disrupt the blood supply. The surface of the pancreas is checked for hemostasis. If there are signs of bleeding, then its sources are coagulated. The lumen of the small intestine is brought to the pancreas along the edges of its resection. The intestine is sutured with separate sutures with an atraumatic needle. The second row is immersed in separate sutures so that the stump of the pancreas, as well as the intestinal wall, covers the end of the pancreas freed from the tissues.
The latter is invaginated into the intestinal lumen, as it were. From our point of view, this is the most favorable type of anastomosis. Despite this, it is advisable to bring two drainage tubes up to 1.0 cm in diameter with holes to the anastomosis (Fig. 116). Precaution is dictated by the possible development of destructive pancreatitis along the seams, which is the reason for the failure of the seams. However, active aspiration can be limited to local peritonitis. Favorable in this situation is that the choledochojejunostomy is located distal, and therefore the flow of bile into the abdominal cavity will be limited if there is no obstacle to its outflow in the distal direction along the intestine. It must be remembered that with a confirmed diagnosis of cancer of the head of the pancreas, the operation should be supplemented with the removal of the omentum and regional lymph nodes.

Fig. 116. The principle of formation of pancreatojejunal anastomosis of the "end-to-end" type
This stage of the operation is performed according to A. Whipple, i.e. up to 2/3 of the stomach is resected. Another type of operation was proposed by Traverso-Zongire (1978) - pancreatoduodenal resection with preservation of the pyloric stomach, or pyloric resection of the pancreas. It was this operation that became an alternative for chronic pseudotumorous pancreatitis with cystic formations in the head. Nevertheless, this type of operation is performed with some difficulties in cancer of the Vater papilla (Tr) and in cancer of the head of the pancreas. The diagram of this operation indicates its complexity. To perform this operation, it is important to preserve the right gastric artery and part of the branches of the right and left gastro-colic arteries. In these situations, the duodenum cannot be crossed below 2 cm, stepping back from the gatekeeper.
The opening of the omental bursa is performed in such a way as to preserve as much of the branch of the right gastro-colic artery as possible. For this, the main part of the greater gland is retained. Of course, this violates the principle of oncology to some extent. The duodenum is visually separated from the edge of the head. Then the restorative-reconstructive stage is carried out in two ways: according to the classical type, i.e. on two loops of the small intestine and on a simplified type - on one intestine. It is important that the supplied bowel loops are located behind the transverse colon.
When performing pancreatoduodenal resection, it is necessary to ensure that the entire complex of resuscitation and intensive therapy is carried out and, above all, the restoration of the volume of circulating blood both during the operation and in the postoperative period. Currently, the volume of blood loss during the operation is fully compensated by the system of the Fresenius apparatus (blood from the surgical wound is sucked into the apparatus and returned to the bloodstream), and in the postoperative period, the replenishment of blood loss depends entirely on the intensity and adequacy of resuscitation measures.
It should be understood that the postoperative wound surface releases a large mass of liquid blood into the abdominal cavity, which must be compensated for during intensive therapy. Failure to replace the volume of circulating blood remained and remains the main cause of death of patients on the 1st - 3rd day of the postoperative period, even with an adequately performed operation. Underestimation of this factor was one of the main causes of death of patients in almost 60% of cases. So, before 1960, mortality after pancreatoduodenal resection of the pancreas was 40-50%. By the 80s. of the last century, it fell to 25%, starting from the 80s-90s. last century - decreased and is 5-12% (VD Fedorov, IM Kuriev, RZ Ikramov, 1999). We obtained approximately the same results in 40 operated patients. The best results were noted by J. Howard et al. - for 199 operations 1% of postoperative mortality, J. Camoron - 145 operations without lethal outcomes.
The question of total resections of the pancreas is very rare. Such messages are casuistic (Fig. 117).

Fig. 117. Total resection of the pancreas, or pancreatectomy
Considering the resection of the pancreas for cysts as a more radical intervention, it should be noted that it is used much less frequently than other types of interventions. This is because mortality and complications do not justify the risk of surgery. Therefore, if you present a diagram of all the main types of operations and the frequency of their use, it will look like this (Fig. 118). At the same time, the radicalism of surgical intervention is sharply reduced with minimally invasive interventions. Such "scissors" in relation to the safety of the operation and radicality in case of oncological alertness justify the use of less traumatic operations. However, they do not provide a high guarantee against relapse. All types of internal drainage are such interventions. This is justified by the fact that the transformation of a cyst into a malignant formation is extremely rare.

Fig. 118. Safety of surgical intervention for pancreatic cysts depending on the volume of the operation (red line): 1 - puncture treatment of cysts; 2 - open drainage; 3 - internal drainage; 4 - resection (various types)
Concluding the consideration of general issues of surgical treatment of pancreatic cysts, it should be noted that the outcomes of operations are not always favorable (recurrence of cysts and the formation of pancreatic fistulas, as well as chronic pancreatitis with frequent exacerbations, significant changes in the function of the pancreas).
I.N. Grishin, V.N. Grits, S.N. Lagodich
Operation technique. It is advisable to open the abdominal cavity with a transverse incision. If necessary, an additional midline incision can be made.
After opening the abdominal cavity, the duodenum and the head of the pancreas are mobilized. To do this, the parietal peritoneum is dissected outside the duodenum and the intestine is stupidly exfoliated together with the head of the pancreas from the retroperitoneal tissue and the inferior vena cava. Exposure of the anterior surface of the head of the pancreas begins with partial intersection of the omentum and gastro-colonic ligament, while ligating the right gastroepiploic artery. The mesentery of the transverse colon is pulled downward, and the stomach upward, the parietal peritoneum is dissected and the mesenteric vessels are separated from the head and uncinate process of the pancreas x. Then mobilize the pyloric part of the stomach along the lesser curvature, ligate and cross the right gastric and gastro-duodenal arteries, displacing the duodenum and the head of the pancreas somewhat downward: the common bile duct and portal vein are isolated.
Pancreatoduodenal resection. Mobilization of the right flexure of the colon
"Atlas of operations on the abdominal wall and abdominal organs" by V.N. Voilenko, A.I. Medelyan, V.M. Omelchenko
Scheme of approaches to the pancreas Isolated lesions of the pancreas are rare. Combined injuries of the gland and other organs of the abdominal cavity are more often observed. Such injuries require urgent surgical intervention. The abdominal cavity is usually opened with an upper midline incision and is approached to the pancreas through the gastrocolic ligament. In the presence of bleeding from a wound in the pancreas, individual bleeding vessels are ligated with catgut. Often ...
End-to-side anastomosis between the gland stump and the small intestine. Suturing the intestine to the posterior wall of the gland stump With the second row of interrupted sutures, the posterior edge of the gland stump is sutured with the posterior lip of the lateral opening of the intestine. After that, in the same way, but in the reverse order, two rows of interrupted sutures are applied to the anterior wall of the anastomosis. Suturing the back lip ...

Destructive forms of pancreatitis complicated by abscess or necrosis of the pancreas are subject to surgical treatment. To reduce the swelling of the gland, its capsule is dissected according to Korte. The abdominal cavity is opened with the upper midline incision, the gastrocolic ligament is dissected, and the anterior surface of the pancreas is exposed. The wound is expanded with mirrors and the abdominal cavity is carefully fenced off with gauze napkins. The capsule of the gland is dissected in the longitudinal direction and ...

